Pressure Injury Prevention
Pressure injuries (PI) impact over 7 million patients per year globally. US healthcare alone reports more than 2.5 million PI cases, over 60 000 deaths, and at least USD 9-11 billion in cost per year.1 Prevention protocols for PI require frequent patient handling and, consequently, contributes significantly to workflow complexity and high incidences of musculoskeletal injuries in healthcare providers, with lower back pain as the dominant on-the-job injury.2 US long-term care centers spend over 6 million USD (56% of all medical costs) every year compensating nurses for occupation-induced back injuries.3
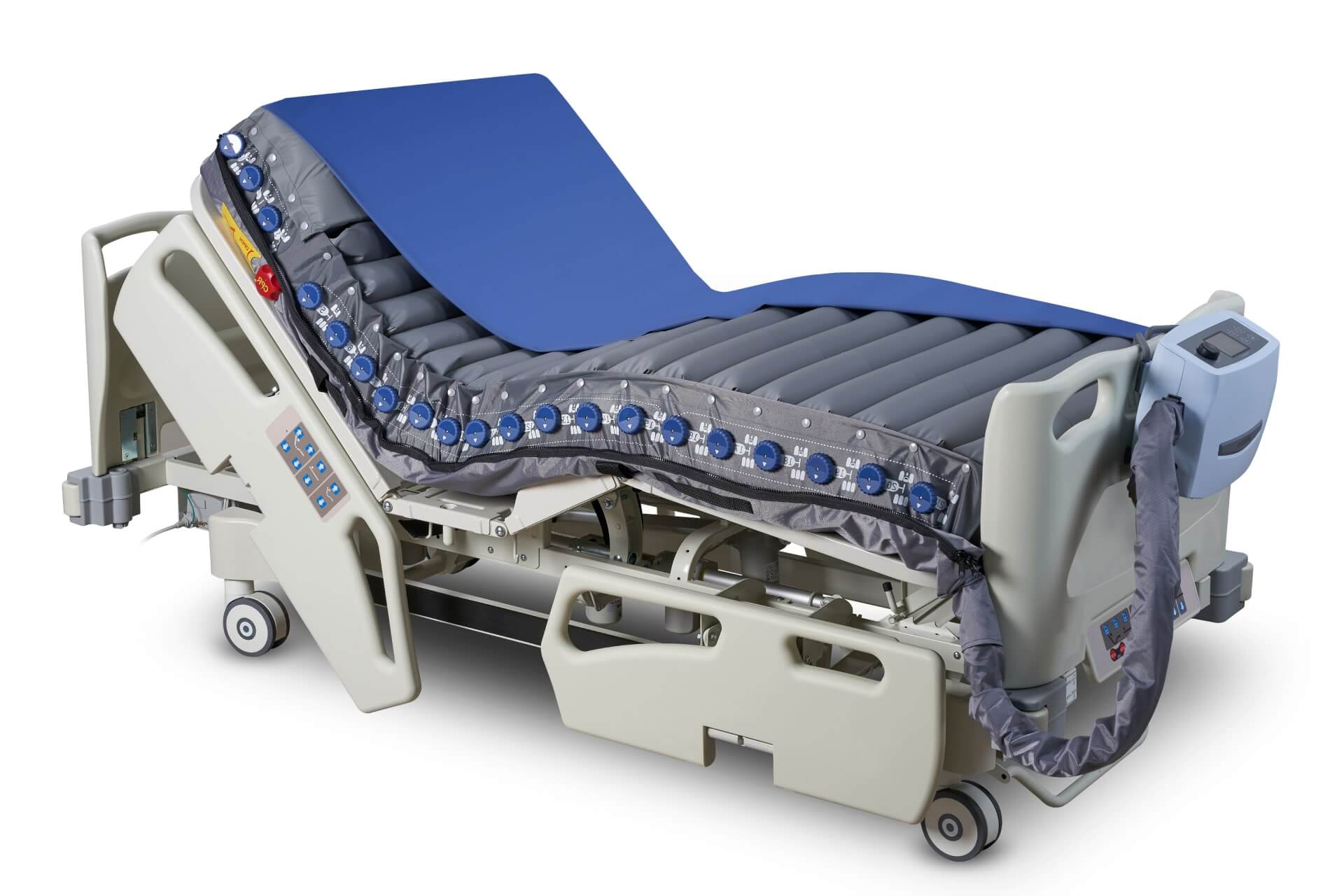
A disproportion between healthcare providers and patient care increases PI and higher incidences of in-hospital post-acute readmission and associated mortality rate.4 Air mattresses that automate labor-intensive procedures and complex therapy workflows, a wide range of pressure settings, and individual air cells that deflate to accommodate unique physical needs, actively prevent PI in post-acute and acute care patients, improving patient outcome and experience, workplace health, and healthcare resource allocation.

Pressure ulcers occur at all risk and care levels.
Up to 50% of acute care and 56% of long-term acute care patients develop pressures ulcers.5 Intervene early.

Ulcers are a prevalent, costly, and global healthcare issue.
Signs of pressure injuries can start to develop during surgeries. When left untreated, injuries become ulcers, and in extreme cases, they can cause death. Pressure redistribution surfaces that aid in turning and repositioning patients improve early interventions.7
Pressure-distributing beds improves cost-effectiveness.
Treatment cost for managing pressure injuries starts at USD 250,000 per inpatient and adds USD 2122 per hospital day.1 Alternating pressure (active) support surfaces improve comfort and reduce pressure ulcers, boosting long-term cost-effectiveness and patient care8


Reference
- Padula, William V et al. “Value of hospital resources for effective pressure injury prevention: a cost-effectiveness analysis.” BMJ quality & safety vol. 28,2 (2019): 132-141. doi:10.1136/bmjqs-2017-007505
- Hignett, S. “Intervention strategies to reduce musculoskeletal injuries associated with handling patients: a systematic review.” Occupational and environmental medicine vol. 60,9 (2003): E6. doi:10.1136/oem.60.9.e6
- Dawson, Anna P et al. “Interventions to prevent back pain and back injury in nurses: a systematic review.” Occupational and environmental medicine vol. 64,10 (2007): 642-50. doi:10.1136/oem.2006.030643
- Burke, Robert E et al. “Hospital Readmission From Post-Acute Care Facilities: Risk Factors, Timing, and Outcomes.” Journal of the American Medical Directors Association vol. 17,3 (2016): 249-55. doi:10.1016/j.jamda.2015.11.005
- Vangilder, Catherine et al. “Results of nine international pressure ulcer prevalence surveys: 1989 to 2005.” Ostomy/wound management vol. 54,2 (2008): 40-54.
- Shafipour, Vida et al. “Prevalence of postoperative pressure ulcer: A systematic review and meta-analysis.” Electronic physician vol. 8,11 3170-3176. 25 Nov. 2016, doi:10.19082/3170
- Black, Joyce M et al. “Pressure ulcers: avoidable or unavoidable? Results of the National Pressure Ulcer Advisory Panel Consensus Conference.” Ostomy/wound management vol. 57,2 (2011): 24-37.
- Shi, Chunhu et al. “Alternating pressure (active) air surfaces for preventing pressure ulcers.” The Cochrane database of systematic reviews vol. 5,5 CD013620. 10 May. 2021, doi:10.1002/14651858.CD013620.pub2